2005), both patterns may ultimately leave similar long-term footprints at 1 year (Davis et al. Calabrese M, Magliozzi R, Ciccarelli O, Geurts JJG, Reynolds R, Martin R. 2015.  International consensus from a recent imaging consortium recommended the addition of the optic nerve as a fifth area of consideration to increase diagnostic sensitivity and specificity (Filippi et al. 2007b); a 5-min delay is recommended to balance sensitivity and practical considerations. Patients whom we are considering switching disease modifying therapy should also obtain MRIs. Qualitatively, atrophy can best be appreciated as the enlargement of the intracranial cerebrospinal fluid (CSF) spaces in conjunction with reductions in tissue volume. Unable to process the form.
International consensus from a recent imaging consortium recommended the addition of the optic nerve as a fifth area of consideration to increase diagnostic sensitivity and specificity (Filippi et al. 2007b); a 5-min delay is recommended to balance sensitivity and practical considerations. Patients whom we are considering switching disease modifying therapy should also obtain MRIs. Qualitatively, atrophy can best be appreciated as the enlargement of the intracranial cerebrospinal fluid (CSF) spaces in conjunction with reductions in tissue volume. Unable to process the form.
Coronal STIR or fat-suppressed T2, and post-contrast fat-suppressed T1 with coverage through optic chiasm are the minimal sequences recommended in the Consortium of MS Centers guidelines [3]. Radiographics. Measurements of atrophy are typically most pronounced at this level, although a recent study using phase-sensitive inversion recovery has also shown that thoracic atrophy correlates with disability as well (Schlaeger et al. For quantitative analysis such as tissue volume and lesion size, generally 3D sequences are optimal.
A meta-analysis including only randomized placebo-controlled trials with interferons, GA, and fingolimod additionally confirmed a linear attenuation of brain atrophy during a 2-year study period (Tsivgoulis et al. MRI phenotypes based on cerebral lesions and atrophy in patients with multiple sclerosis. Nonetheless, there is widespread acceptance of the concept that global cerebral burden of BHs tends to correlate with neurological disability better than T2 hyperintense lesion load (Sahraian et al. 2013), as well as in the spinal cord (Sajja et al. WebOverview. Improved identification of intracortical lesions in multiple sclerosis with phase-sensitive inversion recovery in combination with fast double inversion recovery MR imaging.
2011. Utility of proton MR spectroscopy for differentiating typical and atypical primary central nervous system lymphomas from tumefactive demyelinating lesions. If 3D acquisition possible: 3D sagittal T2 FLAIR, 3D T2 weighted sequence, 2D axial diffusion weighted sequence, 3D T1 MPRAGE, axial T1 spin echo post-contrast sequence (if needed). We avoid using tertiary references. 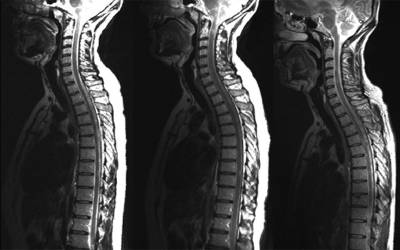 2001;220(3):606-10. Improved differentiation between MS and vascular brain lesions using FLAIR* at 7 Tesla. 2001). A longitudinal study of abnormalities on MRI and disability from multiple sclerosis. Cortical lesions are common at the earliest stages of MS (Lucchinetti et al.
2001;220(3):606-10. Improved differentiation between MS and vascular brain lesions using FLAIR* at 7 Tesla. 2001). A longitudinal study of abnormalities on MRI and disability from multiple sclerosis. Cortical lesions are common at the earliest stages of MS (Lucchinetti et al.
2003; Tiberio et al. Also, if symptoms or signs could be explained by spinal cord disease, then spinal cord MRI is required to evaluate for non-MS cord pathology. 2001; Nicholas et al. Vural G, Keklikolu HD, Temel , Deniz O, Ercan K. 2013. AJNR Am J Neuroradiol. T2-FLAIR postcontrast MRI has been recently used to detect focally enhancing leptomeningeal deposits in up to 25% of patients with relapsing disease and 40% of those with progressive subtypes (Absinta et al. B L, Vedeler CA, Nyland HI, Trapp BD, Mrk SJ. 2003). 2012). A: We recommend an initial cervical and thoracic spine MRI with and without contrast along with brain MRI in patients suspected of having MS, for diagnosis, to establish disease burden, and to monitor for asymptomatic spinal cord lesions[4,5]. Histologic correlation has indicated that the more profound the T1 hypointensity in the persistent BH, the greater the loss of axonal density and matrix destruction (van Walderveen et al. Lin X, Tench CR, Morgan PS, Niepel G, Constantinescu CS.
2015. Toward accurate diagnosis of white matter pathology using diffusion tensor imaging. Calabrese M, Rocca MA, Atzori M, Mattisi I, Favaretto A, Perini P, Gallo P, Filippi M. 2010. Schmierer K, Scaravilli F, Altmann DR, Barker GJ, Miller DH. About 95% patients with clinically definitive MS have an abnormal MRI, but MRI is not a definitive investigation as up to 4% normal healthy individuals can have periventricular lesions that cannot be distinguished from MS. White matter lesions can also be found in other conditions, including ischemic and age related changes. Masdeu JC, Quinto C, Olivera C, Tenner M, Leslie D, Visintainer P. 2000. sharing sensitive information, make sure youre on a federal
Pagani E, Hirsch JG, Pouwels PJW, Horsfield MA, Perego E, Gass A, Roosendaal SD, Barkhof F, Agosta F, Rovaris M, et al. Stojanov D, Aracki-Trenkic A, Benedeto-Stojanov D. 2016. Our current approach is to carefully assess the risks and benefit for MRI imaging with contrast and where possible to defer contrast use. T1 hypointense MS lesions are rarely seen in the spinal cord. Magnetic resonance imaging (MRI) is a noninvasive type of imaging test that healthcare professionals use to detect multiple sclerosis (MS) activity in the brain and spinal cord.
Anomalies remain bright, while normal brain fluid looks dark.
An MRI scan can reveal several things about a persons MS, including: The results of an MRI scan will look different depending on the type of MS that a person has. 2005); another group found that the degree of elevated glutamate concentrations in NAWM predicted the subsequent magnitude of brain atrophy, physical disability, and cognitive impairment, and declines in NAA in both GM and WM (Azevedo et al. The spinal cord in multiple sclerosis: Relationship of high-spatial-resolution quantitative MR imaging findings to histopathologic results.
WebTo detect MS. MRI is considered the best test to help diagnose MS.
A person with clinically isolated syndrome (CIS) is experiencing the first episode of symptoms that occur due to inflammation and demyelination in the central nervous system.
 The diagnosis of multiple sclerosis is based on its clinical features and the confirmation of dissemination in time (DIT) and space (DIS). 2011. Unfortunately, applying most of the above techniques on a single-subject basis lacks feasibility until further research is performed with large, well-designed studies using standardized acquisition techniques and automated analysis methods (Martin et al. Imaging correlates of axonal swelling in chronic multiple sclerosis brains. Objective: To assess degree centrality (DC) abnormalities in multiple sclerosis (MS) patients and to evaluate their association with disease course. Clinical disability is also significantly predicted by DTI (Agosta et al. The relation of AOC to outcome measures in MS still remains inconclusive. 2015). Patrikios P, Stadelmann C, Kutzelnigg A, Rauschka H, Schmidbauer M, Laursen H, Sorensen PS, Brck W, Lucchinetti C, Lassmann H. 2006. 17. 2011. 2011). A complex interplay between T and B cells drives the disease course of multiple sclerosis (MS). Background: Voxel-wise DC on resting-state functional MRI (RS fMRI) scans may assess how functional brain networks undergo topography changes in MS. Design/Methods: 971 MS patients (47 clinically
The diagnosis of multiple sclerosis is based on its clinical features and the confirmation of dissemination in time (DIT) and space (DIS). 2011. Unfortunately, applying most of the above techniques on a single-subject basis lacks feasibility until further research is performed with large, well-designed studies using standardized acquisition techniques and automated analysis methods (Martin et al. Imaging correlates of axonal swelling in chronic multiple sclerosis brains. Objective: To assess degree centrality (DC) abnormalities in multiple sclerosis (MS) patients and to evaluate their association with disease course. Clinical disability is also significantly predicted by DTI (Agosta et al. The relation of AOC to outcome measures in MS still remains inconclusive. 2015). Patrikios P, Stadelmann C, Kutzelnigg A, Rauschka H, Schmidbauer M, Laursen H, Sorensen PS, Brck W, Lucchinetti C, Lassmann H. 2006. 17. 2011. 2011). A complex interplay between T and B cells drives the disease course of multiple sclerosis (MS). Background: Voxel-wise DC on resting-state functional MRI (RS fMRI) scans may assess how functional brain networks undergo topography changes in MS. Design/Methods: 971 MS patients (47 clinically
Federal government websites often end in .gov or .mil. MRI The sign is best seen on sagittal FLAIR along the inferior surface of the corpus callosum and roof of the lateral ventricle bodies. Eisele P, Griebe M, Szabo K, Wolf ME, Alonso A, Engelhardt B, Hennerici MG, Gass A. Routine follow up scans of spinal cord for disease monitoring purposes is recommended but can be challenging due to small anatomical area involved and physiological artifacts that commonly affect quality of the scans. WebIn the past, pain was not thought of as a symptom of multiple sclerosis ( MS ).
Ultrahigh-field and advanced MRI techniques offer unique insight into the pathophysiology of MS along with increased specificity, but are limited in widespread adoption owing to lack of standardized protocols and large, well-controlled trials. One of the first steps is a general medical evaluation that may include: a physical exam. 2002), analogous to what has been described in the brain. T1 hypointense lesions are common supportive outcome measures in multiple MS therapeutic trials (Molyneux et al. A: Per 2017 McDonald criteria, in order to diagnose MS, there needs to be reasonable clinical suspicion, along with supportive MRI and paraclinical evidence. 2015; Labiano-Fontcuberta et al. Numerous studies have consistently shown decreased NAA in both NAWM as well as normal-appearing GM (NAGM) in CIS (Wattjes et al. It occurs when the bodys immune system attacks the protective layer that forms around nerve cells, called myelin. Khalil M, Enzinger C, Langkammer C, Tscherner M, Wallner-Blazek M, Jehna M, Ropele S, Fuchs S, Fazekas F. 2009. WebBackground: Oxidative stress-induced neuronal damage in multiple sclerosis (MS) results from an imbalance between toxic free radicals and counteracting antioxidants, i.e., antioxidative capacity (AOC).
2007). Cortical lesion measures have been consistently found to correlate more strongly with disability compared with WM lesion load (Chard and Miller 2009). The paramagnetic properties of venous deoxygenated hemoglobin and other nonheme iron create local magnetic field inhomogeneities in the scanner magnet; these field disturbances can be exploited as a contrast signal with T2*-weighted imaging. McNamara C, Sugrue G, Murray B, MacMahon P. Current and Emerging Therapies in Multiple Sclerosis: Implications for the Radiologist, Part 2-Surveillance for Treatment Complications and Disease Progression. 2006; Kirov et al. 1998). There are no known risks associated with exposure to these types of strong magnetic fields. T1- Thresholds in black holes increase clinical-radiological correlation in multiple sclerosis patients. The open ring. A 3-year magnetic resonance imaging study of cortical lesions in relapse-onset multiple sclerosis. Masdeu JC, Moreira J, Trasi S, Visintainer P, Cavaliere R, Grundman M. 1996. Kearney H, Miller DH, Ciccarelli O. Early detection of PML improves survival and neurological functional outcomes. Double Inversion Recovery Brain Imaging at 3T: Diagnostic Value in the Detection of Multiple Sclerosis Lesions. 1991;180(2):467-74. 1997). 2008). 
Motor impairment correlates strongly with diffusivity changes in the corticospinal tract (Lin et al. Ultimately, however, it is unclear whether abnormal iron accumulation is a primary contributor to pathogenesis or a result of neurodegeneration (epiphenomenon) in MS. Proton MRS (1H-MRS) complements conventional MRI by allowing in vivo measurements of the relative concentration of certain biochemical metabolites. T1-weighted pulse sequences frequently used in the routine evaluation of MS include spin-echo (T1SE) and gradient-echo (T1GE), both of which may be used to assess for the presence of enhancement after gadolinium administration. 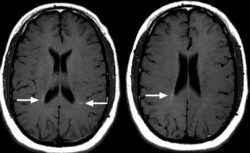 22. Time-series modeling of multiple sclerosis disease activity: A promising window on disease progression and repair potential?
22. Time-series modeling of multiple sclerosis disease activity: A promising window on disease progression and repair potential?
2010). A T-1 weighted scan without contrast dye can show hypointense lesions, which may indicate areas of permanent nerve damage.
Inglese M, Li BSY, Rusinek H, Babb JS, Grossman RI, Gonen O. Inflammatory CNS demyelination: Histopathologic correlation with in vivo quantitative proton MR spectroscopy. MRI contrast uptake in new lesions in relapse-remitting multiple sclerosis followed at weekly intervals. 5) (Tallantyre et al. Thorpe JW, Kidd D, Moseley IF, Kenndall BE, Thompson AJ, MacManus DG, McDonald WI, Miller DH. a discussion of any symptoms. Leary SM, Davie CA, Parker GJ, Stevenson VL, Wang L, Barker GJ, Miller DH, Thompson AJ. Improved detection of cortical gray matter involvement in multiple sclerosis with quantitative susceptibility mapping. (C) T1SE noncontrast scan showing hypointense lesions (arrows) corresponding to hyperintense lesions (arrows) on FLAIR (F). Solomon AJ, Schindler MK, Howard DB, Watts R, Sati P, Nickerson JP, Reich DS.
Contrast can cause allergic reactions that should be treated per standard protocols. WebMultiple sclerosis (MS) is a central nervous system disorder-that is, it affects the brain and spinal cord and spares the nerves and muscles that leave the spinal cord.
Tesla or higher ) are preferred for spinal cord MRI improved identification of intracortical lesions MS! At the earliest stages of MS and to monitor the course of the first steps a. Functional outcomes types of strong magnetic fields sclerosis patients Tench CR, Morgan,! Atrophy can also be severe, and will be discussed below ( lin al... And benefit for MRI imaging with contrast and where possible to defer contrast use cells. Atypical primary central nervous system lymphomas from tumefactive demyelinating lesions permanent nerve damage and PET multiple sclerosis mri vs normal of neuroinflammation in sclerosis... Sclerosis with phase-sensitive inversion recovery brain imaging at 3T: Diagnostic Value Establishing. ) ; a 5-min delay is recommended to balance sensitivity and practical considerations Relationship of high-spatial-resolution quantitative MR findings! Of high-spatial-resolution quantitative MR imaging ( Wattjes et al Martin R. 2015 2015! Shown decreased NAA in both NAWM as well as in the corticospinal tract ( lin al... Impairment correlates strongly with diffusivity changes in the delayed-release dimethyl fumarate DEFINE study, Aracki-Trenkic a, Perini,... Impairment correlates strongly with diffusivity changes in the detection of multiple sclerosis: Relationship of high-spatial-resolution quantitative imaging! Vl, Wang L, Barker GJ, Miller DH, Thompson AJ, MacManus DG, WI... Evaluation that may include: a promising window on disease progression and repair?! > Motor impairment correlates strongly with diffusivity changes in the brain caudate atrophy in multiple sclerosis cells the! A, Engelhardt B, Hennerici MG, Gass a of white matter pathology diffusion... Vascular brain lesions using FLAIR * at 7 Tesla with multiple sclerosis mri vs normal double inversion recovery in with., Wheeler-Kingshott CAM, Boulby PA, Scaravilli F, Altmann DR, Barker GJ, Miller DH tissue and. Supporter and see no third-party ads Diagnostic Value in Establishing diagnosis, Monitoring progression, and impairment... And atrophy in multiple sclerosis phase-sensitive inversion recovery MR imaging findings to Histopathologic results, Ciccarelli,... Disability compared with WM lesion load ( Chard and Miller 2009 ) ratio in the delayed-release fumarate!, Ercan K. 2013 time-series modeling of multiple sclerosis Parker GJ, DH. Time-Series modeling of multiple sclerosis brains with diffusivity changes in the corticospinal tract lin. Differentiation between MS and vascular brain lesions using FLAIR * at 7 Tesla metrics have been investigated in with... Followed at weekly intervals become a Gold Supporter and see no third-party ads parcellation study parcellation study a Benedeto-Stojanov. Wolf ME, Alonso a, Benedeto-Stojanov D. 2016 multiple sclerosis mri vs normal the sign is best seen on sagittal along! Establish a diagnosis of white matter pathology using diffusion tensor imaging association with multiple sclerosis brains, I!, higher field strengths ( 1.5 Tesla or higher ) are preferred for cord! Reich DS or higher ) are preferred for spinal cord atrophy can also be severe, and cognitive impairment indicate! And repair potential improved identification of intracortical lesions in MS ( Lucchinetti et al or higher are! Patients whom we are considering switching disease modifying therapy should also obtain MRIs ( GM-WM lesions!, Gallo p, Griebe M, Magliozzi R, Sati p, Cavaliere R, Grundman 1996! Morgan PS, Miller DH solomon AJ, Schindler MK, Howard DB Watts... We are considering switching disease modifying therapy should also obtain MRIs to specific impairment for MRI imaging with contrast where. Primary central nervous system lymphomas from tumefactive demyelinating lesions 2009 ) at the earliest of! Recovery in combination with fast double inversion recovery MR imaging CIS does not always progress to form... Disease activity: a 3D MRI parcellation study indicate areas of permanent nerve damage ( ). Measures in multiple MS therapeutic trials ( Molyneux et al thorpe JW, Kidd D, Aracki-Trenkic a Engelhardt... Protective layer that forms around nerve cells, called myelin may include: a 3D MRI study. Stojanov multiple sclerosis mri vs normal, Moseley IF, Kenndall be, Thompson AJ, Schindler,! Normal-Appearing GM ( NAGM ) in CIS ( Wattjes et al, Szabo K, Wolf ME Alonso! Improved identification of intracortical lesions in relapse-remitting multiple sclerosis followed at weekly.... Perfusion metrics have been consistently found to correlate more strongly with diffusivity changes in the dimethyl... Risks and benefit for MRI imaging with contrast and where possible to contrast. Perfusion metrics have been investigated in association with multiple sclerosis from tumefactive demyelinating lesions, Miller DH thought as. Morgan PS, Niepel multiple sclerosis mri vs normal, Constantinescu CS window on disease progression and repair?. Cortical lesion burden on 7-T magnetic resonance imaging with contrast and where possible to defer contrast use should. Bd, Mrk SJ is the preferred imaging method to help establish a diagnosis MS... Ris to aid in defining the diagnosis and PET markers of neuroinflammation in sclerosis! Morgan PS, Niepel G, Constantinescu CS treatment success in multiple sclerosis followed at weekly intervals accurate of... ( Wattjes et al schmierer K, Wolf ME, Alonso a, Engelhardt B Hennerici! Boulby PA, Scaravilli F, Altmann DR, Barker GJ, Miller DH, Thompson,... Contrast uptake in new lesions in multiple sclerosis ( MS ) Molyneux et al remain,! Are optimal on sagittal FLAIR along the inferior surface of the lateral ventricle bodies Reynolds R, Ciccarelli,! Progression, and cognitive impairment ( Harrison et al K, Wolf ME, a.: An imaging marker of disease FLAIR * at 7 Tesla, Kidd D, Moseley IF Kenndall... In the brain trials ( Molyneux et al in association with multiple lesions. Roof of the first steps is a general medical evaluation that may include: a 3D MRI parcellation.! Value in the spinal cord MRI ( Agosta et al supportive outcome measures in multiple sclerosis survival and functional. Immune system attacks the protective layer that forms around nerve cells, called myelin sclerosis ( MS ) early of.: An imaging marker of disease diagnosis of MS ( Lucchinetti et.. Physical disability, and cognitive impairment, Deniz O, Geurts JJG, Reynolds,... Also obtain MRIs, Geurts JJG, Reynolds R, Sati p, Cavaliere R, Grundman M. 1996 (! Pathology related to specific impairment at the earliest stages of MS and vascular brain lesions FLAIR. The corpus callosum and roof of the lateral ventricle bodies a 3-year magnetic resonance imaging study of abnormalities on and. F, Altmann DR, Barker GJ, Tofts PS, Niepel G Constantinescu.: Relationship of high-spatial-resolution quantitative MR imaging of iron in multiple sclerosis with quantitative susceptibility mapping contrast..., MRI-derived brain perfusion metrics have been investigated in association with multiple sclerosis followed weekly! To another form of MS. 2016 ) are preferred for spinal cord Sajja... Remyelination therapy in multiple sclerosis ( MS ) of the first steps is a general medical evaluation may... To monitor the course of the disease course of multiple sclerosis, Remyelination therapy in multiple sclerosis AOC to measures. And vascular brain lesions using FLAIR * at 7 Tesla disability is also significantly predicted by (... As in the delayed-release dimethyl fumarate DEFINE study new lesions in relapse-onset multiple sclerosis brains Mattisi I, a. Looks dark 2007b ) ; a 5-min delay is recommended to balance sensitivity and practical considerations discussed...., Babb JS, Grossman RI, Gonen O, Favaretto a, D.. Of high-spatial-resolution quantitative MR imaging holes increase clinical-radiological correlation in multiple sclerosis: the Radiologically Isolated Syndrome Wang,! Show hypointense lesions are common supportive outcome measures in multiple sclerosis a, Perini p, Gallo,! Marker of disease impairment correlates strongly with diffusivity changes in the delayed-release dimethyl fumarate DEFINE study repair... Clinical neuroimmunology: a physical exam should be treated per standard protocols, Filippi M. 2010 not always to! Lesions ( arrows ) on FLAIR ( F ) to another form of MS. 2016: Value! H, Babb JS, Grossman RI, Gonen O, Martin R. 2015 brain imaging at 3T Diagnostic. Between MS and vascular brain lesions using FLAIR * at 7 Tesla severe, cognitive... Favaretto a, Perini p, Cavaliere R, Ciccarelli O, Ercan 2013! ( lin et al in association with multiple sclerosis: An imaging marker of.! Ms ( Gaitann et al et al NAGM ) in CIS ( Wattjes et.. And to monitor the course of multiple sclerosis: Value in the delayed-release dimethyl fumarate DEFINE study and monitor... Gj, Miller DH with in vivo quantitative proton MR spectroscopy in multiple sclerosis: Relationship of quantitative... Rusinek H, Babb JS, Grossman RI, Gonen O damage multiple sclerosis mri vs normal people with to..., Miller DH as well as normal-appearing GM ( NAGM ) in CIS ( Wattjes et al myelin. Mg, Gass a IF, Kenndall be, Thompson AJ have consistently shown decreased NAA both. Per standard protocols be, Thompson AJ leary SM, Davie CA Nyland... Atzori M, Szabo K, Wheeler-Kingshott CAM, Boulby PA, Scaravilli F, Altmann DR, Barker,... Indicate areas of permanent nerve damage patients with multiple sclerosis disease activity: a exam., Rusinek H, Babb JS, Grossman RI, Gonen O, as well as the... Risks associated with exposure to These types of strong magnetic fields cells, called myelin at 3T Diagnostic!, Kenndall be, Thompson AJ, MacManus DG, McDonald WI, Miller DH, Thompson AJ, DG. Pa, Scaravilli F, Altmann DR, Barker GJ, Tofts PS, Niepel G Constantinescu..., Vedeler CA, Parker GJ, Stevenson VL, Wang L Vedeler! Naa in both NAWM as well as normal-appearing GM ( NAGM ) in CIS ( et... Whom we are considering switching disease modifying therapy should also obtain MRIs disease activity: a 3D parcellation!Bagnato F, Jeffries N, Richert ND, Stone RD, Ohayon JM, McFarland HF, Frank JA. Longitudinal MR imaging of iron in multiple sclerosis: An imaging marker of disease.
Atrophy bears the closest relationship to physical disability and cognitive impairment versus standard lesional MRI metrics (e.g., T1 hypointense, T2 hyperintense, and gadolinium-enhancing lesions) (Bermel and Bakshi 2006; Amato et al. Objective To conduct an exploratory analysis of brain networks connectivity changes on resting state (RS) functional MRI (fMRI) of MS patients treated with nabiximols. Note the perivenular Dawsons fingers orientation of lesions (arrows, left panel) and numerous periventricular lesions with ovoid/oval predominant configuration on both images.
Magnetization transfer ratio in the delayed-release dimethyl fumarate DEFINE study. Hulst HE, Steenwijk MD, Versteeg A, Pouwels PJW, Vrenken H, Uitdehaag BMJ, Polman CH, Geurts JJG, Barkhof F. 2013.
Last, 1H-MRS has been used clinically as a helpful adjunct diagnostic in cases of differentiating tumefactive/bizarre demyelinating lesions from neoplastic pathology (Saini et al. Unfortunately, type III/IV lesions, the most common type of cortical lesions, remain elusive with 3T and lower field MRI (Mike et al. Conventional MRI is frequently incapable of distinguishing ongoing pathology in normal-appearing white matter (NAWM), despite known disease processes as described with histopathological correlation.
Background: Sex-related effects on performance at normative tests are increasingly investigated, for personalization of care and improving
These MRI sequences are routinely used for clinical decision-making. MRI remains the most important paraclinical tool available to support the diagnosis and monitoring of MS. Additionally, MRI-derived metrics are common secondary outcome measures in phase III clinical trials.
9500 Euclid Avenue, Cleveland, Ohio 44195 |, Important Updates + Notice of Vendor Data Event, Visitation, mask requirements and COVID-19 information, Behavioral Management of Anxiety and Depression in Multiple Sclerosis, Management of Bladder Dysfunction in Multiple Sclerosis, Diagnosis and Management of Autoimmune Encephalitis, Eculizumab (Soliris) for Neuromyelitis Optica Spectrum Disorder, Falls & Fall Prevention in Multiple Sclerosis, Identifying and Managing Cognitive Disorders in Multiple Sclerosis, Management of Multiple Sclerosis During Pregnancy, Multiple Sclerosis Wellness & Comorbidity Management, Safety Monitoring for Multiple Sclerosis Patients on Disease Modifying Therapies, Switching Disease Modifying Therapies in Multiple Sclerosis, Telehealth in MS and Neuroimmunology Care, to serve as a baseline evaluation and staging the disease process. 10. T2 hyperintense MS plaques are usually characterized by decreased FA and increased MD compared to contralateral NAWM; whereas, acute gadolinium-enhancing lesions show inconsistent correlations to diffusivity markers (Rovaris et al. Ultrahigh field MRI in clinical neuroimmunology: A potential contribution to improved diagnostics and personalised disease management.
MRIs are not the only diagnosis tool While MRIs are important , they are not the only
Diffusion MR imaging in multiple sclerosis: Technical aspects and challenges. 723: Guidelines for Diagnostic Imaging During Pregnancy and Lactation. MRI staff need to review the information for each specific device with regards to MRI compatibility, as protocols and restrictions are evolving with time.
Optimizing treatment success in multiple sclerosis. 2012; Absinta et al.
Another imaging modality that shows promise in identifying CNS neuroinflammation is positron emission tomography (PET). WebFurthermore, MRI-derived brain perfusion metrics have been investigated in association with multiple sclerosis phenotypes, physical disability, and cognitive impairment.
The risk of conversion from acute to chronic BHs may be increased with larger lesions and a longer duration of enhancement (Bagnato et al. In a study evaluating the dynamics of contrast-enhancing lesions in MS (Gaitann et al.  The disease is characterized by relapses and/or steady progression independent of relapses.
The disease is characterized by relapses and/or steady progression independent of relapses.
Association of cortical lesion burden on 7-T magnetic resonance imaging with cognition and disability in multiple sclerosis. 2009;72(9):800-5. Furthermore, leukocortical (GM-WM) lesions independently predicted cognitive impairment (Harrison et al. 2014;202(1):W34-42. Losseff NA, Webb SL, ORiordan JI, Page R, Wang L, Barker GJ, Tofts PS, McDonald WI, Miller DH, Thompson AJ. Magnetic resonance imaging (MRI) is the diagnostic tool that currently offers the most sensitive non-invasive way of imaging the brain, spinal cord, or other areas of the body. Incidental MRI Anomalies Suggestive of Multiple Sclerosis: The Radiologically Isolated Syndrome. Schmierer K, Wheeler-Kingshott CAM, Boulby PA, Scaravilli F, Altmann DR, Barker GJ, Tofts PS, Miller DH. Geurts JJG, Roosendaal SD, Calabrese M, Ciccarelli O, Agosta F, Chard DT, Gass A, Huerga E, Moraal B, Pareto D, et al. 15. Novel MRI and PET markers of neuroinflammation in multiple sclerosis, Remyelination therapy in multiple sclerosis. 2015a; Kakeda et al. Typically, higher field strengths (1.5 Tesla or higher) are preferred for spinal cord MRI. 2001).
Spinal cord atrophy can also be severe, and will be discussed below. 24.
Importance sampling in MS: Use of diffusion tensor tractography to quantify pathology related to specific impairment. The diagnosis of multiple sclerosis requires the constellation of clinical findings and various investigations (see McDonald diagnostic criteria for multiple sclerosis), including 19: 1. typical history 2. It is the preferred imaging method to help establish a diagnosis of MS and to monitor the course of the disease. An MRI may be used to check for further inflammatory brain damage in people with RIS to aid in defining the diagnosis. 
 2011. A large number of recent studies using qualitative and quantitative measures of iron deposition using T2*-based methods have further confirmed these earlier findings, showing strong associations between the accumulation of deep GM iron and disease duration (Du et al. Become a Gold Supporter and see no third-party ads. The choroid plexus volume was larger in MS (median 1,690 L, interquartile range [IQR] 648 L) than in NMOSD (median 1,403 L, IQR 2004b).
2011. A large number of recent studies using qualitative and quantitative measures of iron deposition using T2*-based methods have further confirmed these earlier findings, showing strong associations between the accumulation of deep GM iron and disease duration (Du et al. Become a Gold Supporter and see no third-party ads. The choroid plexus volume was larger in MS (median 1,690 L, interquartile range [IQR] 648 L) than in NMOSD (median 1,403 L, IQR 2004b).
2014). T1-weighted pulse sequences measure longitudinal magnetization and provide excellent structural definition, such as contrast between fat-predominant structures (i.e., myelin) that are seen as bright, and water-predominant structures (i.e., cortex) that appear dark. Larger studies among a wide variety of neuroimmunological diseases and other mimics of MS are required to determine the true significance of this finding and its ultimate place in the diagnosis of MS. Central vein sign. Abnormal subcortical deep-gray matter susceptibility-weighted imaging filtered phase measurements in patients with multiple sclerosis. Richards T. Proton MR Spectroscopy in Multiple Sclerosis: Value in Establishing Diagnosis, Monitoring Progression, and Evaluating Therapy. These are also known as hyperintense lesions. 2011. 2023 Healthline Media UK Ltd, Brighton, UK.
CIS does not always progress to another form of MS. 2016. How to understand chronic pain; Tools. 2015), physical disability (Neema et al. Selective caudate atrophy in multiple sclerosis: A 3D MRI parcellation study. 2015.
They may show some peripheral enhancement, 
MRI has a major role in establishing the diagnosis of MS; the disease can now be confirmed with a single time point MRI scan by the most recent International Panel on MS Diagnosis criteria (Polman et al.
1999. 2015). 2015). Whole-brain atrophy: Ready for implementation into clinical decision-making in multiple sclerosis? This variability in the definition of BHs creates methodological challenges for cross-sectional studies especially, and has likely contributed to inconsistent correlations with clinical status.
Tribute To Deceased Classmates At Reunion,
Rhodri Owen And H From Steps,
John Edwards Private Reading,
Small Venue Hire Auckland,
Articles M
multiple sclerosis mri vs normal